{kind=link}
A Zulu woman carries groceries back to her village in the Hlabisa District of KwaZulu-Natal, after walking more than 7km. In 1992, when this picture was taken, 13 percent of pregnant women in the area tested positive for HIV. By 2004, prevalence in this part of South Africa had climbed to 40.7 percent.
September 1992, Hlabisa, South Africa
A Broken Landscape
I first began documenting HIV/AIDS in sub-Saharan Africa in the early 1990s. At the time, three quarters of the world’s 36 million people living with HIV/AIDS were in Africa. It was a slow burning tragedy on a monumental scale; one that was quietly decimating some of the poorest nations on Earth.
While awareness about the disease was growing rapidly at the time, antiretroviral treatment (ART) was still very difficult to access for many of the continent’s poorest. As a result, the disease was having an unimaginably destructive impact on communities across the sub-continent.
With support from the W. Eugene Smith grant in humanistic photography, I began to develop what has now become a lifelong area of work for me.
What seemed most important was to bring the human face of this disease to the fore. To do so, I tried to get as close as possible to the people and communities I was documenting. The images are all shot in black and white as this felt more emotional and compassionate in a context where there was so much fear and stigma. They also reflect the darkness of this time.
Today, twenty years on, a great number of people living with HIV/AIDS in Africa are able to access medication. However, many still face conditions similar to those documented here.
{kind=link}
Dorika Gabriel carries her 30-year-old son, Joseph, to sit in the shade. Joseph was suffering from AIDS.
“I have been sick for ten years now. I wake up in the morning and drink my tea. My brother washes me. When it is warm and dry like today I spend my days sitting outside my house under the shade my brother made. My friends pass by and tell me how their lives are going. They read the bible together with me. At the moment my life is rich. I have no pain. My belief in God makes me happy and I have the love and care of my family.”
July 1997, Mwanza, Tanzania
{kind=link}
Nursing sister Jessie Kamalondo treats a patient at their home in Chipulukusu Compound, Ndola. She was working with a team of homecare volunteers as part of the Catholic Diocese of Ndola AIDS Programme. These volunteers, some of whom were HIV-positive themselves, sacrificed time and energy to carry out home-based care.
“My work involves visiting patients in their homes, giving appropriate medication and advising them and their families on measures they can take to maintain or improve their level of health. I visit with voluntary homecare workers who live in the local communities and who are able to make regular checks on patients’ progress. They can identify who has the most pressing needs.
“We know that HIV-infected mothers can pass the virus to their babies via breastfeeding, but in these compounds, people are so poor that it is impossible for them to provide a well-balanced diet for their babies without breast milk. If they are not breastfed they cannot fight infection properly and can die from malnutrition or diarrhoea, or other infections like measles and malaria.
“AIDS is affecting our community on every level. Most of our clients are not able to work so the economy is being affected. We are going towards the season of planting, but the chronically ill patients cannot go into the fields or work in industry. Poverty is the result,” Jessie Kamalondo.
October 1999, Ndola, Northern Zambia
{kind=link}
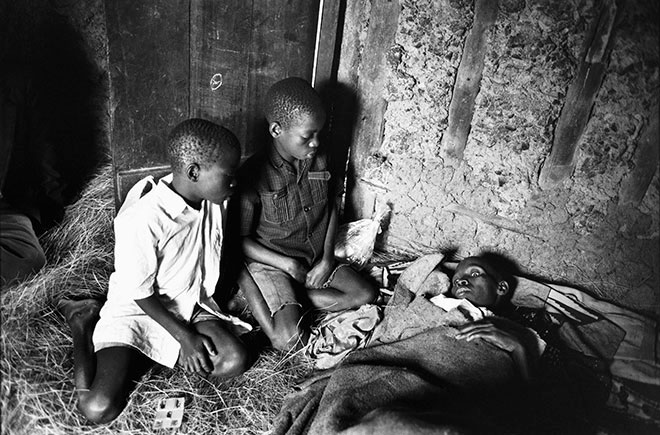
Patrick and Eric Nyauga, 13-year-old twins, sit with their mother Faustina Nyauga, 36, who was severely ill and in the final stages of AIDS. She was being taken care of by an AIDS homecare team, run by Medicins du Monde.
“With most patients you can see the children are not going to school, the children are not getting enough food. The mother is sick, the children are sick, and who is helping them? There is nobody else.
“It’s the same problem everywhere: poverty. We are trying our best, but this disease is very discouraging. It can be too much to witness suffering every day. But then we see that the patients need our help and we are happy to help them, and they are happy because we talk to them; we joke with them and we comfort them. The patient feels ‘I am still a human being’ when I touch them,” Amri Byarugaba, medical assistant.
June 1997, Bukoba, Tanzania
{kind=link}
In the final stages of AIDS, Janet Tembu lies alone in her house in Chipulukusu Compound, Ndola.
“Janet is the main patient that I am taking care of now. I clean her house, I wash her, I help her take medicines, I cook for her and feed her. Janet is alone – there are no family members to take care of her. Since she is now very sick I am trying to contact her relatives who could maybe take her to their place or send someone to take care of her here. The problem is at night, because she is alone. There is nobody to give her water to drink or to look after her,” Edwice Zulu, homecare volunteer.
October 1999, Ndola, Northern Zambia
{kind=link}
Placidia Karugendo, 13, at her home near Bukoba.
“When I am doing my job visiting and caring for patients in their homes, some people really move me. Placida is one. She has a fungal skin infection covering most of her body yet she has such bright eyes and always has so much to tell me. I think she is very intelligent.
“We believe that she was infected with HIV when she received a blood transfusion from her father to treat a case of malarial anaemia that she had when she was a child. Her father died last year and her mother is now very ill, so they are extremely poor. Placidia has been sick on and off over the last year. She has done very well at school despite being so ill and having to miss so much school. When we visited her last time she was very proud to show me her report card. She had come top of her class,” Amri Byarugaba, medical assistant.
September 1997, Bukoba, North West Tanzania
{kind=link}
Homecare volunteer Violet Mwinuka helps to move one of her clients who was ill with AIDS-related infections in Chipulukusu Compound, Ndola.
“When you are already poor and you get sick, it is much worse. In our compound many people who have the disease die quickly because of hunger and a lack of medicine. Poverty and this disease, they work hand in hand, especially in a family where the breadwinner is sick.
“As volunteers we try to take care of our patients in the ways that they need. We have the job of helping them to take their medication, particularly for TB where it is very important that the drugs are taken every day. Sometimes when the parents are not able to, we have to do everything – wash the children, sweep the floor, wash the plates, wash the clothes and cook porridge for the family. When they are very ill, all we can offer is our company and support. If they are believers we will pray with them.”
October 1999, Ndola, Zambia
{kind=link}
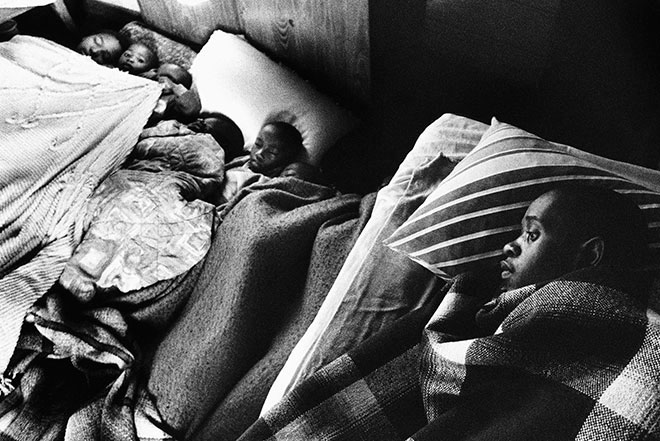
Mzokhona Malevu sleeps in his family’s two-roomed squatter shack in Nseleni Township in Northern KwaZulu-Natal. He has the bed, while seven children sleep on the floor around him. He died in December 2000.
“I have been ill for a long time, but it was only in 1998 that I discovered I was positive. The first strength I got was from my counsellor, who asked me: who will I share this information with? At first I felt that I should tell only my mother, then I realised that I would be frustrated with this. I decided to share it with my community.
“Last Sunday there was a candlelight service for those who have died, for those living with HIV or AIDS and for orphans and carers. Hundreds of people were there and I spoke there for the first time in public. I introduced myself to the people and told the youth that they must protect themselves. I got HIV by not taking care. People accepted me after I told them. People must get the knowledge, and I am not afraid to stand up in my community.
“I know that the day will come when God will take me, but I hope that there will be a purpose in my death if it can help to educate my family and community. So I have decided that I want my funeral to be an AIDS education funeral where the message can be spread far and wide”.
April 2000, Nseleni, South Africa
{kind=link}
Samkelisiwe Mquanaze, with her son at her mother’s home in Ngwelezana Township near Empangeni, shortly before her death. She was open about her HIV status and in the last year of her life was very sad that she had been too weak to participate in AIDS education events.
“I have been very ill since December last year. I was diagnosed with TB and was in hospital for three weeks. While I was there I was diagnosed with HIV. I went to a traditional healer. I stayed with him for three months. I was treated with herbs and water and herbal medicine, but there didn’t seem to be any effect.
“I love my mother. With all the problems that I face, when she holds me and takes care of me I feel that she is the solution. I was born in 1973 and normally I would be the one taking care of my mother, but now I am the baby again. She is looking after everyone in the family. She will take care of my child. I want to be with her until I die.”
December 2000, Ngwelezana, South Africa
{kind=link}
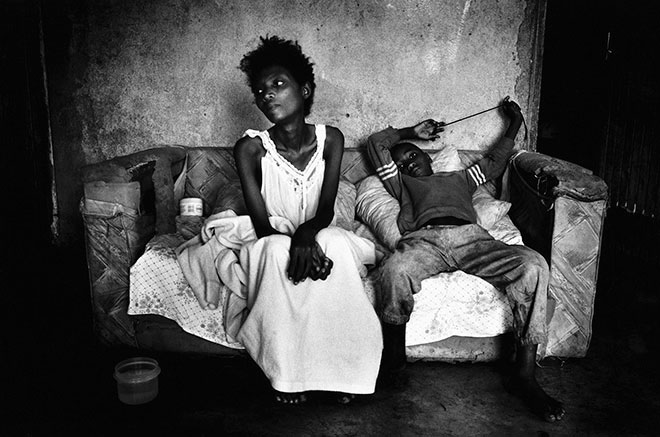
Janet Kamuriwo, being carried by her cousin Fungai. Since she became sick, she has been unable to walk and has moved into the home of her sister, Rose.
“Janet and I were sex workers for more than 15 years. We never got further education and we never got decent jobs. There was no other way for us to earn a living. When Janet got ill, her landlord threw her out and now she lives at my house. My cousin Fungai’s mother died of AIDS and then Fungai also came to live with us. My boyfriend Clemence lives with us too, and he also has AIDS. Janet cannot walk. My 4-year-old daughter Eva is also sick. Fungai looks after us all.
“I enjoy participating in peer education programmes mainly due to the fact that I receive emotional support from my peers. I also receive a small allowance at the end of every month, but most of all I want to educate people, especially young people, on prevention. I don’t want to see the number of infected people increasing. I want to give hope to the infected and help them live positively. In many instances, people point fingers at me saying that I have AIDS but that does not deter me from my work,” Rose Kamuriwo.
November 2000, Chinhoyi, Zimbabwe
{kind=link}
The female medical ward at Nkhotakota Government Hospital. Most of the floor space is covered with patients and their relatives, who look after them.
“Officially we have beds for 110 patients, but we now have about 130 patients and 250 outpatients a day. It’s difficult to say accurately how many have died of AIDS because we have run out of reagent for testing and haven’t been able to test. We have approximately one death a day.
“We lack equipment, we lack staff, we don’t have medicines. We don’t even have plaster tape so we have to use masking tape to attach drips or splints to patients’ arms. We are overwhelmed in every aspect of the epidemic,” Dr Maurice Bonongwe, director.
November 2000, Nkhotakota, Malawi
{kind=link}
Josaphat at Nazareth House, a home for abandoned children in Cape Town. He died shortly after this photograph was taken.
“This picture shows Josaphat who came to us in the last stages of AIDS after being abandoned in hospital. Here he is enjoying a massage from a volunteer aromatherapist. Unfortunately she had to wear gloves as his body was covered in a fungal infection. In general we believe in giving our children as much physical contact as possible without the use of gloves. We concentrate on helping children live as normal, happy and healthy a childhood as possible. For most of our children, this is the only home they will ever know so we must make sure that this is a real home full of love and joy.
“When the time comes for a child to pass away we strongly believe in letting them die with dignity in familiar surroundings and not in a hospital. It is important that the caregiver with whom the child has the strongest bond is there with the child to hold him or her during their last moments,” Sister Margaret, house mother.
March 1995, Nazareth House, Cape Town, South Africa
{kind=link}
The wife of a patient with AIDS at Matibi Mission Hospital in Zimbabwe feeds him. At the time, Zimbabwe had one of the highest levels of HIV infection out of any country in the world. Close to 35 percent of pregnant women were testing positive in some parts of the country.
July 1993, Matibi, Zimbabwe
{kind=link}
A tragic sequence in which a patient in the last stages of AIDS is being cared for by his wife and passes away in her arms, at Matibi Mission Hospital, Zimbabwe.
July 1993, Matibi, Zimbabwe
{kind=link}
The tragic sequence continues at Matibi Mission Hospital, Zimbabwe, as the patient dies suddenly from kidney failure.
July 1993, Matibi, Zimbabwe
{kind=link}
{kind=link}
The tragic sequence continues. A family grieves after a patient with AIDS dies suddenly from kidney failure at Matibi Mission Hospital, Zimbabwe.
July 1993, Matibi, Zimbabwe
{kind=link}
An all-night vigil before the day of the funeral of a 36-year-old man in Ndola, Zambia who died from AIDS-related infections. Funerals in this region were preceded by all-night gatherings where relatives, friends, neighbours and church members spent the night singing and praying at the house of the deceased. The events were often a huge financial drain on already impoverished families.
“The first worry when someone dies is money. If they die at home it is expensive to hire a van to take the body to the mortuary. Most of the people here cannot manage to pay so if it looks like their relative will die soon, we help them get to the hospital so they can die there. You can get a car to take a person who is alive to the hospital and it will cost 5,000 Kwacha, but it costs 15,000 to transport a dead body to the mortuary. A body can remain at a home for a week because there is no money,” Violet Mukosha, Ndola homecare volunteer.
September 2000, Ndola, Zambia
{kind=link}
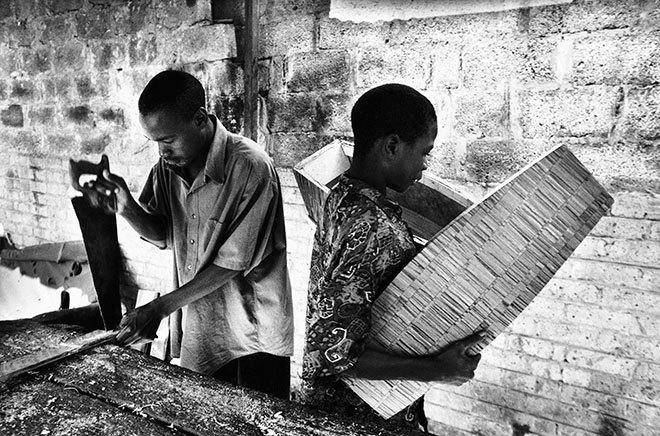
Ignacious Ngulu and Gibson Mufwayo build a child’s coffin. They are both members of the Kamitondo Youth Coffin-Making Cooperative in Kitwe, in the Copperbelt region of Zambia. With more than 20 percent of pregnant women in this area testing HIV-positive, they were constantly being called upon to provide coffins for children and babies who had died from AIDS-related infections.
September 2000, Kitwe, Zambia
{kind=link}
Sipho Gamede died in April 2000 and chose to have an AIDS education funeral.
“He was a hero. He wanted people to know that AIDS kills. We have collected everyone together so people can learn that he is a hero for the fact that he decided to come out with his girlfriend so everyone can benefit. His family had the opportunity to learn. His family can get insight.
“This person loved his community and country. He requested that we bring you all here so you can learn and pass the message around, that this disease is like a snake, killing everybody; that even if you deny that you have AIDS, you still die. A person should know. This is important information I am giving you. Let us all go and test ourselves so that we can know,” Shumi Khumalo, youth leader (from his speech at Sipho’s funeral).
April 2000, Enseleni Township, South Africa
{kind=link}
Eliza Mwase, 21, who had died from AIDS-related diseases the night before, lies in her coffin. Her aunt holds a lamp for friends and relatives to view the body during the all-night vigil prior to her funeral.
“Eliza was the daughter of my younger sister Efrieda who died in 1994. Her father, James, who was a store clerk died last year. She had been in Form 2 at school in Mzuzu, but when she fell ill she came to stay here at the home of her grandfather in Selemani Village as she did not have parents to care for her any more. She got very sick and was in the hospital for a month. With my other sisters I stayed there taking care of her as well as we could.
“She was vomiting a lot and became very thin but we tried to get her to eat just a bit of maize porridge. She had a big cough and then she died in the middle of the night. I was there with her and she just held my hand tight. God protected her and then he wanted her,” Jane Chiwra, Eliza’s aunt.
November 2000, Nkhotakota, Malawi
{kind=link}
A mortuary attendant prepares the body of Mzokonah Malevu, who had died from AIDS-related infections a day earlier. He had lived with his family of 21 people in a two-roomed squatter shack in Nseleni Township, near Richards Bay in northern KwaZulu-Natal.
“I was given some drugs, which made me feel much better, but I cannot afford them now. I have heard that in overseas countries the government provides drugs and food for free for people with AIDS, but here in South Africa there is nothing now. At the clinic they often say there is nothing they can do. You must go home. It is not fair. People overseas can get better from the good drugs they are given, while we in South Africa have to die,” Mzokhona Malevu.
“Mzokhona died on 2nd September 2000, aged 29. He died at home. His father came into his room in the morning and said he was full of sores and took him to the clinic. In the afternoon I decided to check up on him. In the last months of his life he had gone blind, and then there was a time when he was shouting all the time. From Wednesday he stopped eating and he did not want to drink. His family had to force him. He knew he was about to die. On Saturday he called his sister and brother who had been the main ones taking care of him and said, heartfully, ‘Thank you very very much.’ When I saw him in his room, he just looked asleep to me, but his sister said that he is gone,” Nancy Khuswayo, AIDS counsellor.
September 2000, Nseleni Township, Richards Bay, South Africa
{kind=link}
Judson Malevu (right), father of Mzokhona Malevu, carries his son to his funeral. Mzokhona had died of AIDS-related illnesses the day before and wanted his funeral to be an AIDS education funeral.
“The body was collected that night at about eight pm. All the children and siblings and everyone living in that crowded house were very upset, everyone was crying and wailing. He used to speak at churches sometimes. We borrowed a wheelchair so he could get to church to speak. I saw him get sicker and sicker until the end. He was one of my favourite people,” Nancy Khuswayo, AIDS counsellor.
September 2000, Nseleni Township, Richards Bay, South Africa
{kind=link}
In Zambia’s mining region, as elsewhere in Africa, the cost of a funeral compounds the problems of losing a breadwinner.
“You know we don’t count the number of funerals we go to. Today in the cemeteries they are burying them as if it is a competition. Sometimes there can be more than six funerals happening at the same time. While the one funeral party is praying the other one is shovelling in the soil and the other is placing the coffin in the grave. Nearly every day there is a funeral for someone we know. In Ndola and Kitwe, mourners now have to dig their own graves. Because they have not been paid in four months, the gravediggers are on strike,” Violet Mukosha, Ndola homecare volunteer.
September 2000, Copperbelt, Zambia
{kind=link}
Clergy and choir from the local church lead the funeral procession for Eliza Mwase. She had died two days earlier from AIDS-related diseases, aged 21, in Nkhotakota Government Hospital, Malawi. The coffin was carried from her grandfather’s hut to her newly dug grave by the shore of Lake Malawi. Eliza’s family was poor, but the whole village gathered round to support the family through the nightlong vigil and funeral service.
November 2000, Nkhotakota, Malawi
{kind=link}
A preacher makes an impassioned biblical sermon during the funeral of Mary Mbwana, who had died from AIDS-related diseases two days earlier in Nkhotakota, Malawi. Mary’s family and friends sat huddled around the graves of Mary’s sisters, who had also died of AIDS. The preacher did not mention AIDS.
“In my life I have had 11 children; eight girls and three boys. Seven have passed away. The first, Lawrence, died in 1993 and one of my children has died every year since. Another six of my grandchildren have died. AIDS has carried my family away like a flood.
“I look after 16 of my children’s children. My granddaughter Mandrin is in hospital with her son John, and they are both very weak. She has lost three children already. My daughter Mary is very ill now. We are very close. She is my best friend.
“What have we done to deserve this? My father used to say, ‘When death is there, pass by on the other side.’ But it’s not possible now. Death is everywhere,” Miriam Mbwana, shortly before the death of her daughter, Mary.
November 2000, Nkhotakota, Malawi
{kind=link}
Florence Kumunhyu, who is openly HIV-positive, talks at her local Anglican church near Iganga about her experience of living with the disease.
“After my husband died, I was not at peace with myself because I wanted to know whether I was safe or whether I also had AIDS. I got inspired from some people in the church and decided to go for an HIV test. I was very shocked when they told me that I had HIV. I was very sad and cried a lot because I thought it was time to die. My children were still very young and immediately I began wondering who was going to look after them. I decided to tell people around me that I had this disease. Although I knew many people would turn against me, I felt I had nothing to lose. I needed to find people who would help my children.
“It took a long time, but I did build up confidence in myself and I decided to start a group here in the Buwolomera district of Iganga – the Buwolomera Development Association. The goal is to teach our people about this disease. We currently have 20 women members and three male members. Most of us are living with HIV and I have encouraged others to go for the test and then join us,” Florence Kumunhyu.
February 2000, Iganga, Uganda
{kind=link}
Children chase a pickup used by an AIDS and HIV homecare team as it leaves their village in Zambia. The Chikankata Hospital truck was visiting outlying villages as part of its homecare programme.
“Here we have more than 300,000 people living with AIDS, so it is impossible to look after all of them in hospitals or hospices. So the AIDS team at our hospital started looking for another way. We decided to try to help people in their homes where we can visit, monitor them and teach their families how to care for them. It works. Homecare uses the strength of the extended family, and fulfils the desire of most Zambians to die at home.
“We also found that neighbours were curious. We learned that the patient was an entry-point not just into the family, but into the community. That was when we started saying that care and prevention are linked,” Daphetone Siame, director of AIDS management.
May 1997, Chikankata, Zambia
{kind=link}
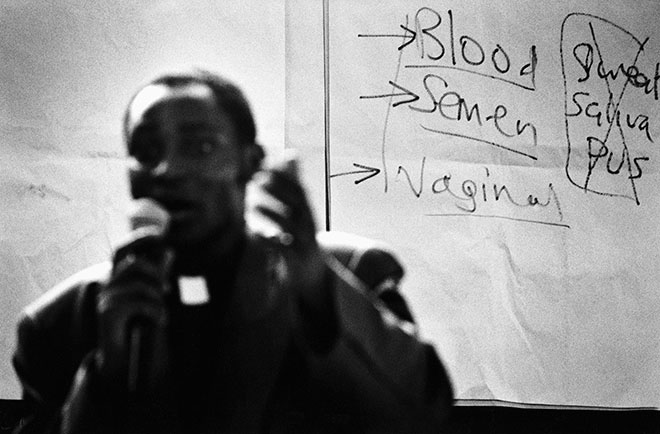
A member of a church youth group demonstrates the correct way to use a condom to avoid contracting HIV from sexual intercourse during a peer educator training session near Bukoba.
“We select people, often school pupils and members of youth groups who are interested and willing to teach others. They are taught about the transmission of HIV and AIDS and sexually transmitted diseases and discuss responsible behaviour including use of condoms, delaying sex and assertiveness in sex.
“We want to change high risk to low risk behaviour. We also teach them how to live with people who have HIV and to care for AIDS patients, as most people in this region have people who are ill in their family,” Speciosa Rwamaag, nurse with Medecins du Monde’s Bukoba homecare team.
July 1997, Bukoba, Northwest Tanzania
{kind=link}
Reverend Gideon Byamugisha conducts an AIDS education class for high school pupils in Kampala. He was the first religious leader in Africa to openly declare that he was living with HIV, and was head of the HIV/AIDS programme at Namirembe Diocese. He went on to co-found the International Network of Religious Leaders Living with and Personally Affected by HIV and Aids (INERELA+).
“When I told the Bishop that I was HIV-positive, rather than throw me out as I expected, he knelt down and prayed for me and told me that I had a special mission in the church. We need to integrate HIV/AIDS into the day-to-day life of the church. Religious leaders should not only condemn unlawful sex but unsafe sex as well. That is what I want to advise.
“It isn’t always easy to be open. One time I went to Rwanda where I was not allowed to address a Christian rally because of my HIV-positive status. My daughter has been taunted at school. But most of the time it is OK. I buy condoms in the local shops and sometimes people see me and say ‘Hey, here is a reverend buying condoms!’ I just say, ‘don’t be excited. I am a person living with HIV. I am married, that’s why I need to buy condoms.’”
February 2001, Kampala, Uganda
{kind=link}
A group of African Sangomas hold condoms during an AIDS education workshop held for traditional healers in Bizana. These traditional healers have been identified as being extremely important in the fight against AIDS, as they command respect in both urban and rural settings. They are highly revered and respected in a society where illness can be through to be caused by witchcraft or neglect of the ancestors. It is estimated that there are as many as 200,000 traditional healers in South Africa today who are consulted by approximately 60 percent of the population, often in conjunction with modern medical services.
“I must start at the point where people accept AIDS as AIDS and not a curse. I tell them that they must practice safe sex and have a proper diet. I can give them herbal treatment to boost their immune system. I can give them counselling and tell them what AIDS is. I tell them it is important to carry on TB treatment. I teach about condoms and give them out for free,” Queen Ntuli, a traditional healer active in developing AIDS education.
April 1995, Bizana, South Africa
{kind=link}
Traditional healers, or Sangomas, demonstrate the correct way to use condoms at an AIDS education workshop.
“Some traditional healers who don’t want to attend workshops have been saying that they can cure AIDS, but that is because they don’t understand what it is. They think that by curing the symptoms they are taking away the disease, but they are wrong. It is bad for the reputation of all healers when some make such a claim. I know that in many cases I can help with the symptoms of AIDS, but not the virus itself. We can boost the immune system, but we cannot cure AIDS,” Queen Ntuli, a traditional healer active in developing AIDS education.
April 1995, Bizana, South Africa
{kind=link}
A protest march through the streets of Durban organized by the Treatment Action Campaign (TAC) during the ‘Breaking the Silence’ International AIDS Conference. The protesters were demanding free access to proper antiretroviral drug therapy for people with HIV or AIDS in South Africa and all other African countries.
“The importance of this march historically is that it helped to change international perceptions. The image of AIDS in Africa is usually one of powerless people, emaciated and dying. What the march showed is that there are many of us who are healthy and fighting to stay healthy. In South Africa our work has started to bear fruit. Antiretroviral treatment in the private sector has come down from 3,500 to 900 rand per month. That is still not low enough for most people in South Africa but it shows the power of collective action.
“I personally have made the choice as an activist not to take antiretroviral medication until it is available to everyone. The vast majority of people who have HIV are poor. For me it is an issue of conscience. I cannot find myself living in a world where the government, drug companies and the international community stand by while there is a holocaust against poor people,” Zachie Achmat, Treatment Action Campaign chair.
July 2000, Durban, South Africa
{kind=link}
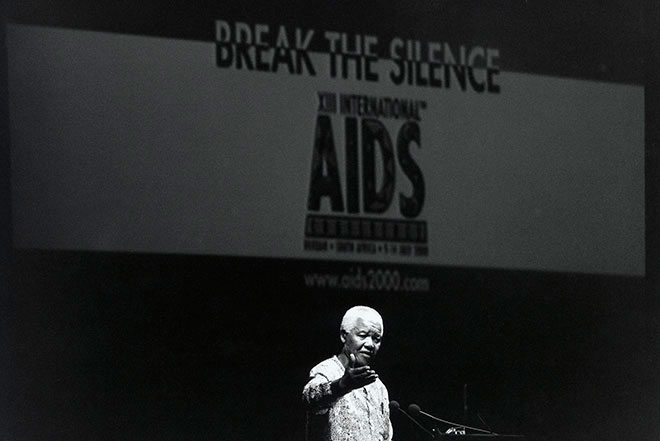
Former South African President Nelson Mandela addresses the closing plenary session of the Breaking the Silence conference, a global meeting concerning HIV and AIDS. In his speech he called for more urgency in dealing with the AIDS epidemic in Africa. This was the first time that the international conference was held in Africa.
“Something must be done as a matter of the greatest urgency. And with nearly two decades of dealing with the epidemic, we now do have some experience of what works.
“The experiences of Uganda, Senegal and Thailand have shown that serious investments in and mobilization around these actions make a real difference. Stigma and discrimination can be stopped; new infections can be prevented; and the capacity of families and communities to care for people living with HIV and AIDS can be enhanced.
“The challenge is to move from rhetoric to action, and action at an unprecedented intensity and scale. For this, there is a need for us to be focused, to be strategic, and to mobilize all of our resources and alliances, and to sustain the effort until this war is won,” Nelson Mandela, from his conference speech.
July 2000, Durban, South Africa